Quick Answer
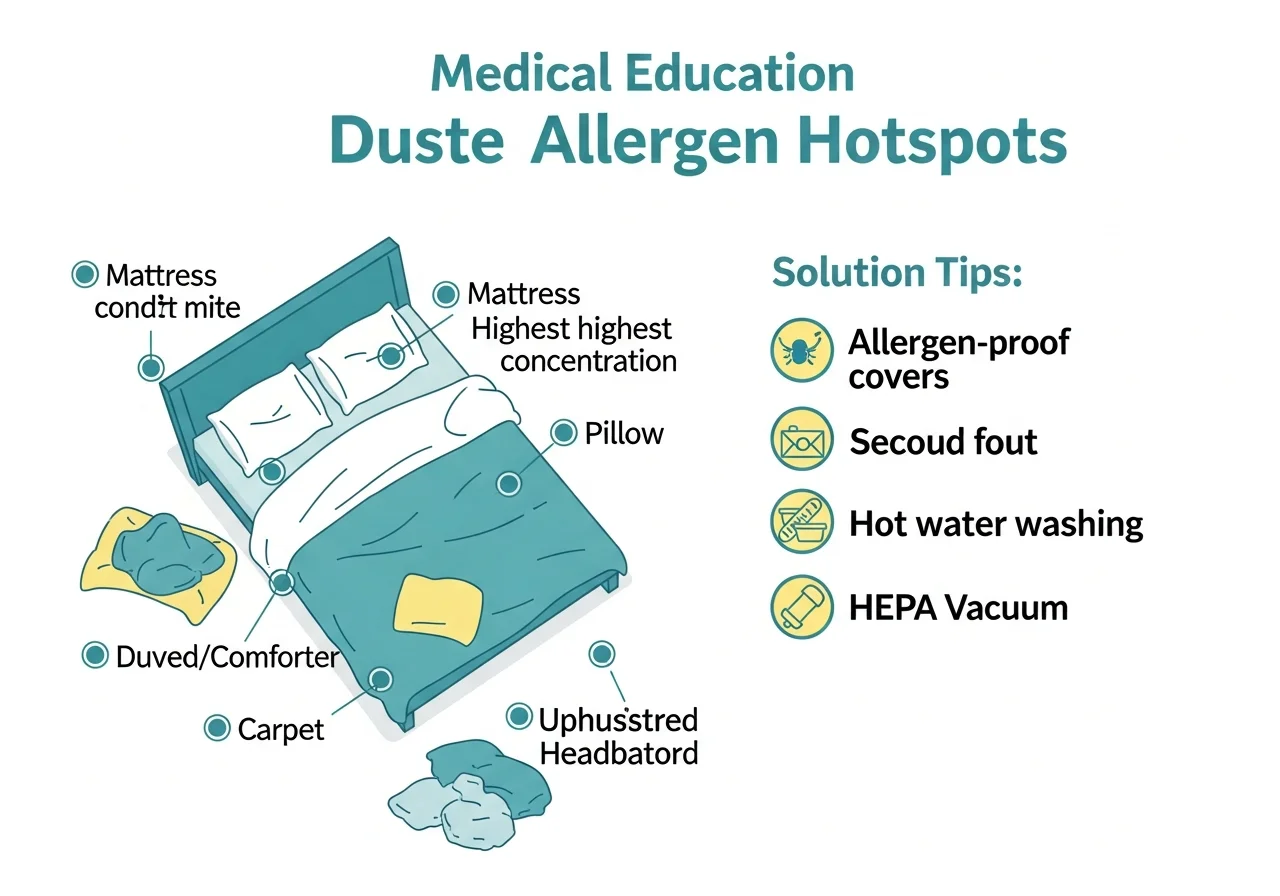
Dust mite allergy causes year-round rhinitis, asthma, and eczema worsening — with symptoms often worst in the morning and after disturbing bedding or upholstered furniture. The allergens are fecal pellets and body fragments of microscopic Dermatophagoides mites. Allergen-impermeable bedding covers, hot water laundering, humidity control, and HEPA vacuuming are the most effective environmental controls.
Dust Mite Allergy Symptom Checklist
Why Dust Mite Allergens Are So Pervasive
House dust mites are one of the most clinically significant aeroallergen sources worldwide, sensitizing an estimated 1 billion people globally. Their primary allergens — Der p 1 and Der p 2 (D. pteronyssinus) and Der f 1 and Der f 2 (D. farinae) — are proteases and lipid-binding proteins that directly cleave tight junctions in airway and conjunctival epithelium, disrupting the mucosal barrier and facilitating allergen penetration. This barrier disruption explains why dust mite allergy is so strongly linked to both rhinitis and eczema. Understanding how allergens trigger the immune system explains why sensitized individuals react even to low allergen exposures.
Dust Mite vs Seasonal Allergy: How to Tell Them Apart
The most distinguishing feature of dust mite allergy is its year-round, perennial pattern without seasonal variation. Pollen allergies improve or resolve when pollen season ends. Dust mite allergy persists throughout the year, is worse indoors (especially the bedroom), often worst in the morning upon waking, and improves when the patient spends extended time away from home. Humidity strongly influences symptom severity — dry winter air reduces mite populations but increases nasal mucosal dryness; humid summer conditions increase mite growth and allergen production.
Formal allergy testing with skin prick testing or specific IgE blood testing to dust mite extracts definitively distinguishes mite allergy from other causes of perennial rhinitis including pet allergy, mold allergy, and non-allergic (vasomotor) rhinitis.
When Dust Mite Allergy Symptoms Are Serious
- Asthma exacerbations: Dust mites are the single most common indoor asthma trigger — inadequate dust mite control in asthmatic households is strongly associated with increased hospitalizations and emergency visits
- Severe eczema: Dust mite sensitization is a major contributor to difficult-to-control atopic dermatitis — barrier disruption by Der p 1 protease directly worsens skin disease
- Chronic sinusitis: Persistent mite-driven nasal inflammation predisposes to recurrent sinus infections requiring ENT evaluation
- Sleep disruption: Nighttime nasal congestion from dust mite allergy can contribute to sleep-disordered breathing, including obstructive sleep apnea worsening
Environmental Control Strategies
| Intervention | Effectiveness | Notes |
|---|---|---|
| Allergen-impermeable mattress/pillow covers | High | Most evidence-based single intervention; reduces allergen 50–80% |
| Weekly hot wash of bedding (≥60°C/140°F) | High | Kills mites and removes allergen from linen |
| Indoor humidity below 50% | High | Mites cannot survive below 50% relative humidity |
| HEPA vacuum cleaner | Moderate | Reduces surface allergen; prevents aerosolizing during vacuuming |
| Remove bedroom carpets | Moderate-High | Carpet holds 100x more allergen than hard flooring |
| Wash stuffed toys weekly | Moderate | Children's toys are significant reservoirs |
| Air filtration (HEPA) | Low-Moderate | Captures airborne particles; small adjunctive benefit |
Treatment Overview
Environmental controls form the foundation of dust mite allergy management but are rarely sufficient alone for significantly sensitized patients. Medical treatment follows the same framework as other aeroallergen allergies: antihistamines for symptom control, intranasal corticosteroid sprays for chronic nasal inflammation, and inhaled corticosteroids for asthma. Allergen immunotherapy for dust mites has strong evidence from randomized controlled trials — both subcutaneous (allergy shots) and sublingual (drops/tablets) approaches are clinically validated for D. pteronyssinus and D. farinae. See our complete treatment guide for all options, and our severe allergies overview for cases where symptoms significantly impact quality of life.